By Dr. Walter Zamarian Jr. — CRM-PR 17,388 | RQE 15,688 | Member of SBCP and ASPS. Last reviewed: May 24, 2026.
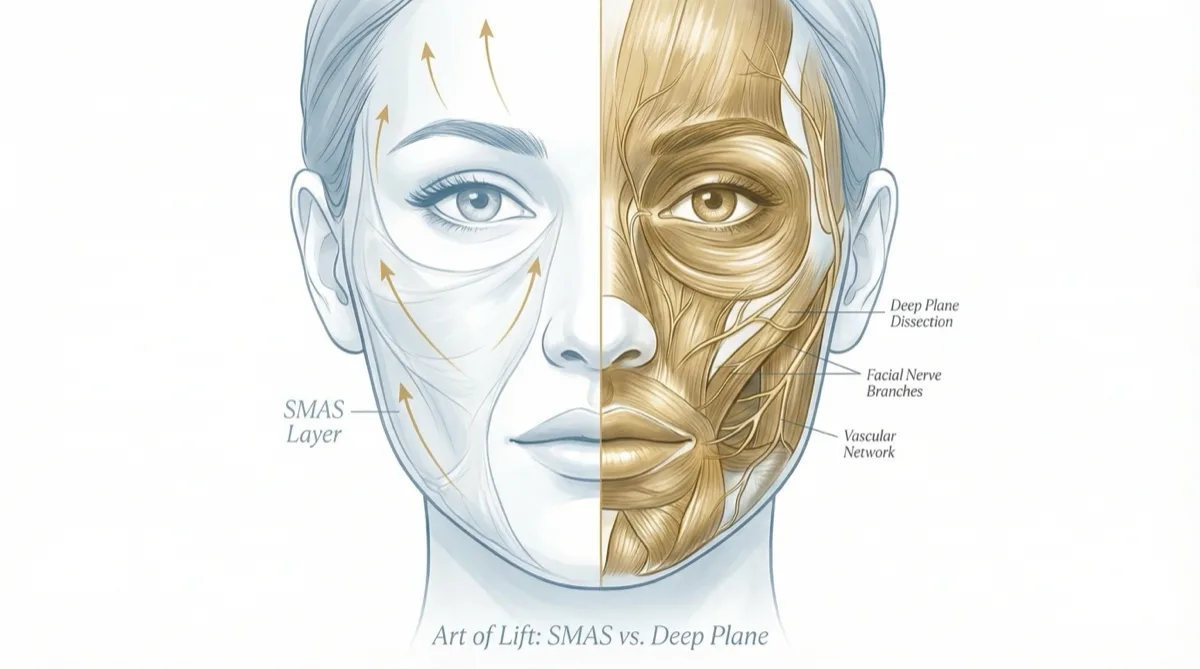
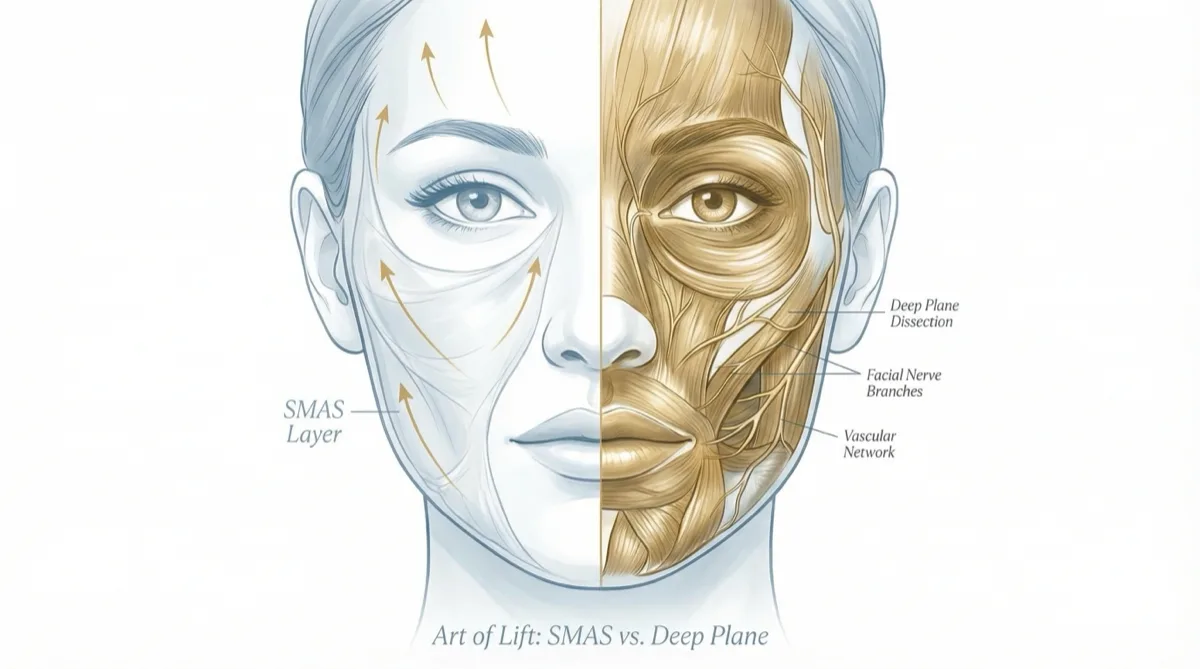
Deep Plane and SMAS facelifts are not competing brand names; they are different surgical ways of mobilizing facial soft tissue. SMAS techniques tighten or reposition the superficial musculoaponeurotic system, while a Deep Plane facelift works beneath the SMAS and releases selected retaining ligaments so the cheek, jawline, and neck can be repositioned with less skin tension. Neither technique is automatically right for every patient.
The right choice depends on anatomy, facial aging pattern, skin quality, neck laxity, previous surgery, medical history, recovery planning, candidate selection and the surgeon.s experience with the technique being proposed. This article explains the difference in plain English while keeping the surgical details accurate enough for patients comparing options, including sub-SMAS/deep-plane dissection, scar placement, scar visibility and candidate selection.
What is the SMAS layer?
SMAS stands for superficial musculoaponeurotic system. It is a fibrous layer beneath the facial skin and superficial fat, connected to deeper facial structures and involved in facial expression and soft-tissue support.
In many SMAS facelift techniques, the surgeon tightens, folds, imbricates or repositions this layer, then redrapes the skin. SMAS-based procedures can be appropriate for many patients and remain part of modern facelift surgery. The important question is not whether SMAS is “old” or “bad,” but whether the technique addresses the patient’s specific anatomy without excessive skin tension.
What is a Deep Plane facelift?
A Deep Plane facelift works in a deeper anatomical plane, beneath the SMAS. The surgeon releases selected facial retaining ligaments, such as zygomatic and masseteric retaining ligaments, so the cheek and jawline tissues can move as a more integrated unit.
This approach is especially relevant when midface descent, jowling, nasolabial fold depth and neck contour are part of the same aging pattern. Because the repositioning is carried by deeper tissues rather than the skin alone, the goal is a more natural vector of lift and less visible pull on the skin.
My approach to Deep Plane surgery has been shaped by formal plastic surgery training, more than 20 years of practice, more than 8,000 surgeries, and continued learning from Dr. Tim Marten and Dr. Mike Nayak in the United States during ASAPS Meetings. That continuing education informs technique, but it does not replace individualized assessment and careful surgical judgment.
Deep Plane vs SMAS: the practical differences
| Question | SMAS facelift | Deep Plane facelift |
|---|---|---|
| Main layer addressed | SMAS layer is tightened or repositioned. | Dissection goes beneath the SMAS in selected areas. |
| Retaining ligaments | Often less direct release, depending on technique. | Selected ligaments are released to mobilize deeper soft tissue. |
| Skin tension | Can vary; too much skin tension may look pulled. | Designed to place more support on deeper tissues and less on skin. |
| Midface | May improve indirectly or modestly, depending on technique. | Can be stronger for cheek descent and nasolabial fold support when indicated. |
| Neck and jawline | Can improve jowls and jawline in selected patients. | Often planned with neck lift or deep neck work when cervical aging is present. |
| Recovery | Varies by extent, anesthesia and patient factors. | Also variable; deeper dissection does not automatically mean a harder recovery. |
| Longevity | Depends on anatomy, technique, aging, skin quality and habits. | May be durable in well-selected patients, but aging continues and no fixed duration should be promised. |
Is Deep Plane always better than SMAS?
No. Deep Plane is not automatically better than SMAS for every face. A patient with early laxity, limited midface descent or a need for a smaller correction may not need the same operation as someone with heavier jowls, cheek descent and neck laxity.
The strongest surgical plan is usually the one that matches the anatomy. For some patients, that may be a SMAS-based facelift, mini-facelift or limited neck procedure. For others, especially when the aging pattern involves the cheek, jawline and neck together, a Deep Plane plan may offer a more complete anatomical correction.
Why retaining ligaments matter
Facial retaining ligaments act like anchoring points between deeper structures and superficial soft tissue. When the cheek and jowl descend with age, simply pulling skin or tightening a superficial layer may not fully address these tethering points.
Deep Plane surgery releases selected ligaments so the soft tissues can move in a more vertical and anatomical direction. This is one reason the technique is discussed so often in relation to midface rejuvenation and natural-looking facial movement.
How this fits regenerative facial planning
Many patients do not age in only one layer. They may have deep soft-tissue descent, neck laxity, eyelid skin excess and volume loss at the same time. In those cases, Deep Plane surgery can be planned alongside Regenerative Deep Plane, blepharoplasty and facial fat grafting when each component has a clear indication.
Fat grafting should be described responsibly. Transferred fat can restore selected areas of volume, and adipose tissue contains stromal and adipose-derived cells that are being studied for their biological properties. That does not make facial fat grafting a stem-cell therapy, and it should not be sold as a guaranteed way to regenerate skin.
Recovery: what patients should expect
Recovery after either technique depends on the extent of surgery, anesthesia, bleeding tendency, smoking, skin quality, revision history and whether eyelids, neck or fat grafting are added. Many patients plan for roughly two weeks away from highly visible social or work commitments, but some need more time and some return sooner to low-demand activities.
Swelling, bruising, tightness, numbness and temporary asymmetry can occur. Patients should know the warning signs that require contact with the surgical team: sudden swelling, worsening one-sided pain, active bleeding, fever, drainage, skin color change, shortness of breath, chest pain, calf swelling or new neurologic symptoms.
For a deeper recovery discussion, read the safety and risk guide: Deep Plane facelift risks, and the longevity guide: how long Deep Plane facelift results may last.
Questions international patients should ask
International patients comparing facelift options in Brazil should ask practical questions, not just marketing questions:
- Is the surgeon a board-certified plastic surgeon with a valid RQE?
- Where is the surgery performed, and what anesthesia support is used?
- Which anatomical findings make Deep Plane or SMAS appropriate in this case?
- Will the neck, eyelids or facial volume need separate planning?
- How long should the patient stay in Londrina before flying home?
- Who monitors the early postoperative period and warning signs?
- What is the plan if revision surgery has been done before?
Online consultation can start the discussion and help determine whether travel is reasonable. A final surgical indication still requires in-person examination before any operation.
Frequently asked questions
Is SMAS outdated?
No. SMAS facelift techniques remain valid and can be appropriate for selected patients. The question is whether the chosen method matches the patient’s anatomy, expectations, risk profile and desired degree of correction.
Does Deep Plane last longer?
Deep Plane results may be durable in well-selected patients because deeper tissues carry more of the support, but no surgeon should promise a fixed number of years. Aging continues, and longevity depends on anatomy, technique, genetics, sun exposure, smoking, weight changes and follow-up care.
Is Deep Plane recovery harder?
Not necessarily. Deeper anatomical work does not automatically mean a harder recovery, but the total recovery depends on the extent of surgery and whether neck lift, blepharoplasty or fat grafting are added.
Can Deep Plane be used in revision facelift?
Sometimes, but revision cases require particular caution because scar tissue, altered anatomy and previous vectors change the surgical plan. Patients considering repeat surgery should read more about revision facelift and discuss timing carefully.
How I make the decision
I do not choose Deep Plane because it is fashionable, and I do not dismiss SMAS because it is older. I choose based on anatomy. In the consultation, I assess the cheek, jawline, neck, skin quality, volume loss, previous procedures, health history and the patient’s ability to follow recovery instructions.
Dr. Walter Zamarian Jr. is a plastic surgeon in Londrina, Brazil, with CRM-PR 17,388 and RQE 15,688. He is a member of the Brazilian Society of Plastic Surgery and the American Society of Plastic Surgeons, with more than 20 years of experience and more than 8,000 surgeries performed. Learn more about his training and background.
If major weight loss or GLP-1 medication has changed facial volume, the planning may also involve tissue repositioning and volume restoration. Read the related guide: Facelift after Ozempic and fat grafting.