Structural rhinoplasty and preservation rhinoplasty are not competing recipes, and one technique is not automatically better than the other. The safer choice depends on dorsal anatomy, tip support, septum, breathing, skin thickness, asymmetry, previous surgery and the degree of change the nose needs.
Patients often hear these terms online and assume they must choose a label before consultation. In reality, the surgeon’s job is to diagnose the anatomy first and then choose the technique, or combination of techniques, that protects function and creates a natural balance with the face.
Medical review
Written and reviewed by Dr. Walter Zamarian Jr., plastic surgeon in Londrina, Brazil. CRM-PR 17.388, RQE 15.688, full member of the Brazilian Society of Plastic Surgery (SBCP) and member of the American Society of Plastic Surgeons (ASPS). 20+ years of experience and 8,000+ surgeries performed. Last reviewed: May 24, 2026.
What is structural rhinoplasty?
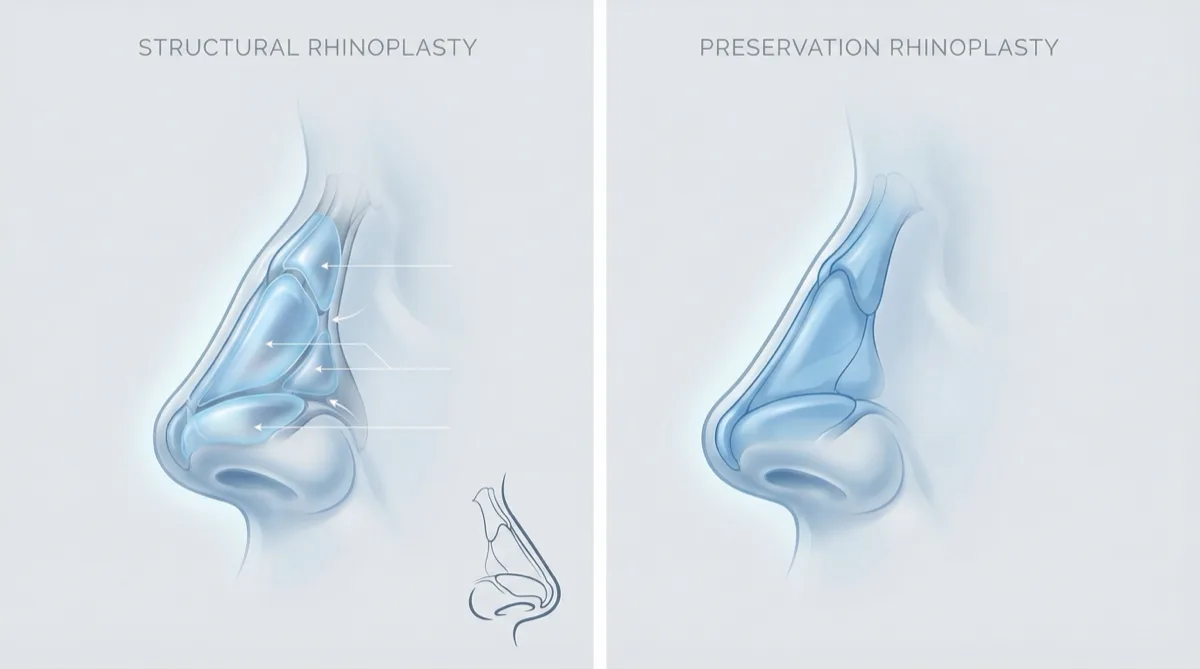
Structural rhinoplasty is a philosophy that rebuilds and supports the nasal framework when support is weak, deviated, asymmetric or previously altered. The operation may be open or closed, but it often uses cartilage grafts to shape and reinforce the nose.
Cartilage usually comes from the septum. In selected revision or complex cases, ear or rib cartilage may be needed. Grafts such as spreader grafts, septal extension grafts, columellar struts or tip grafts can support breathing, projection, rotation and symmetry when native structures are not enough.
Structural planning is especially useful when the nose has a significant septal deviation, weak tip support, collapse of the middle vault, previous surgery, trauma, marked asymmetry or a need for meaningful change in projection or definition.
What is preservation rhinoplasty?
Preservation rhinoplasty tries to maintain more of the natural nasal architecture, especially the dorsal aesthetic lines, instead of removing and reconstructing the bridge in a traditional way. Techniques such as push-down or let-down lower the nasal dorsum while preserving selected structures.
This approach may be appropriate when the dorsal shape is favorable, the septum is stable, the tip does not need major support, asymmetry is limited and breathing anatomy allows a conservative plan. In the right patient, preservation principles can reduce dissection and maintain natural contours.
Preservation is not a shortcut and it is not suitable for every nose. Significant deviation, weak support, severe asymmetry, thick skin with poor definition, airway compromise or prior surgery may require structural reconstruction.
Structural vs preservation rhinoplasty: practical comparison
| Question | Structural planning | Preservation planning |
|---|---|---|
| Core idea | Rebuild and support the framework when needed | Preserve selected native structures when anatomy allows |
| Dorsum | May reshape, reconstruct or reinforce the bridge | May lower the bridge with push-down or let-down concepts |
| Tip | Allows stronger support and definition when the tip is weak | Works when the tip needs limited modification |
| Septum and breathing | Useful when septal deviation or valve weakness must be corrected | Requires careful selection when the septum is stable |
| Revision surgery | Often needed when anatomy has been altered | May be limited after previous surgery |
| Recovery | Swelling may last months, especially in thick skin or complex cases | Some selected patients may have less early swelling |
Hybrid rhinoplasty is often the real answer
Modern rhinoplasty is not always purely structural or purely preservation. Many cases use preservation principles where the anatomy is favorable and structural support where the nose needs reinforcement. This hybrid mindset is often more realistic than defending one label for every patient.
For example, a patient may benefit from preserving dorsal lines while using structural grafts to improve tip support or the internal nasal valve. Another may need a more complete structural plan because breathing, deviation or previous surgery makes preservation unsafe or insufficient.
Breathing, septum and function come first
Rhinoplasty should not be planned only from profile photographs. The septum, turbinates, internal nasal valve, external valve, skin thickness and previous trauma all matter. When breathing is part of the complaint, septorhinoplasty planning may be necessary.
Techniques that look elegant in diagrams can fail if the functional anatomy is ignored. A smaller bridge, narrower bones or more defined tip should not come at the cost of nasal obstruction.
When structural rhinoplasty may fit better
- Revision rhinoplasty or previous nasal trauma.
- Significant septal deviation or valve collapse.
- Weak tip support or poor tip definition.
- Marked asymmetry or crooked nose.
- Need for projection, rotation or support using cartilage grafts.
- Selected ethnic rhinoplasty cases where support and definition must be built carefully.
For related planning, see revision rhinoplasty, ethnic rhinoplasty and the guide on when revision rhinoplasty may be needed.
When preservation rhinoplasty may fit better
- A favorable dorsal shape with a limited hump.
- A stable septum and no major airway complaint.
- A well-supported tip that needs conservative refinement.
- Limited asymmetry and no major previous surgery.
- Patient goals that fit a conservative anatomical change.
Recovery and swelling
Recovery depends more on the amount of dissection, bone work, skin thickness, grafting, bleeding tendency and whether the case is primary or revision than on the label alone. Preservation rhinoplasty may reduce early swelling in selected cases, but it does not eliminate swelling or make recovery uniformly faster.
Structural rhinoplasty can involve more grafting and support work, so swelling may take longer to settle, especially in thick skin. Final definition can take many months. Tools such as ultrasonic rhinoplasty may be considered for selected bone work, but they do not replace surgical judgement.
Risks and red flags
Risks of rhinoplasty include bleeding, infection, septal perforation, poor wound healing, visible or unfavorable scarring, skin problems, graft visibility, graft warping or resorption, asymmetry, persistent swelling, nasal obstruction, changes in smell, dissatisfaction, need for revision and anesthesia-related complications.
Urgent postoperative signs include rapidly increasing pain, fever, pus, heavy bleeding, skin color change, worsening obstruction, visual symptoms, shortness of breath, chest pain or neurologic symptoms. These require immediate contact with the surgical team or emergency care.
Frequently asked questions
Is preservation rhinoplasty automatically better because it is newer?
No. Preservation rhinoplasty is valuable for selected anatomy, but newer terminology does not replace diagnosis. Some noses need preservation principles, some need structural support, and some need both.
Does open rhinoplasty always leave a visible scar?
No, but no surgeon should promise an invisible scar. The columellar incision often heals subtly when well placed and cared for, but scar visibility depends on skin, healing, tension, sun exposure and individual biology.
Can rhinoplasty be combined with chin surgery?
Yes, in selected patients. Nose and chin balance strongly affects the facial profile, so chin implant or mentoplasty may be discussed when chin projection changes how the nose is perceived.
How I choose the technique
In consultation, I evaluate photographs, nasal bones, dorsal lines, tip support, septum, valves, skin, breathing, previous surgery and expectations. 3D simulation can help communication, but it is not a promise of outcome. The final plan is anatomical: structural, preservation or hybrid, depending on what your nose safely allows.
Read Also

Dr. Walter Zamarian Jr.
Plastic surgeon in Londrina, Brazil (CRM-PR 17.388 | RQE 15.688), full member of SBCP and ASPS. He has worked in plastic surgery for more than 20 years, with a focus on individualized planning, patient safety, Deep Plane facelift, structural rhinoplasty, and female intimate surgery.
Follow this blog on Google
Want to find more articles from this blog on Google? Add Dr. Walter Zamarian Jr. to your preferred sources.
Deixe um comentário